
Shangjie Lai writes about the role of migration in transmission routes of malaria between sub-Saharan Africa and China.
The international spread of infectious diseases including Plasmodium falciparum malaria has been accelerated by increasing human mobility via air travel over recent decades. An emerging route of P. falciparum infection is from Africa to China by Chinese migrant workers, threatening the health of travelers and challenging the National Malaria Elimination Action Plan (2010-2020), which aims to eliminate malaria by 2020. A paper I recently published with colleagues in Scientific Reports sought to quantify the patterns of malaria importation to China from sub-Saharan Africa (SSA) and explore the key driving factors. Risk factors behind the high mortality rates in imported cases were also examined.
Characteristics of P. falciparum cases imported from SSA to China.
From 2011 to 2015, a total of 8,653 P. falciparum malaria cases recorded in China were imported from SSA, with an overall 5-year incidence rate of 6.5 cases per one million persons. The median age of patients was 40 years old (Interquartile range [IQR] 31–46) with a strong male predominance (27.7:1). The African migrant cases (258) only accounted for 3.0% of all imported cases, and most were Chinese (97.0%). 91.3% of cases were Chinese migrant workers with a median duration of stay in SSA of 317 days (IQR 168–496). The spatial distribution of imported cases in China varies substantially (Figure 1), with the highest density in the counties of Guangxi province of southern China, Jiangsu and Anhui provinces in eastern China, and Sichuan provinces in western China (≥ 50 cases per one million persons).
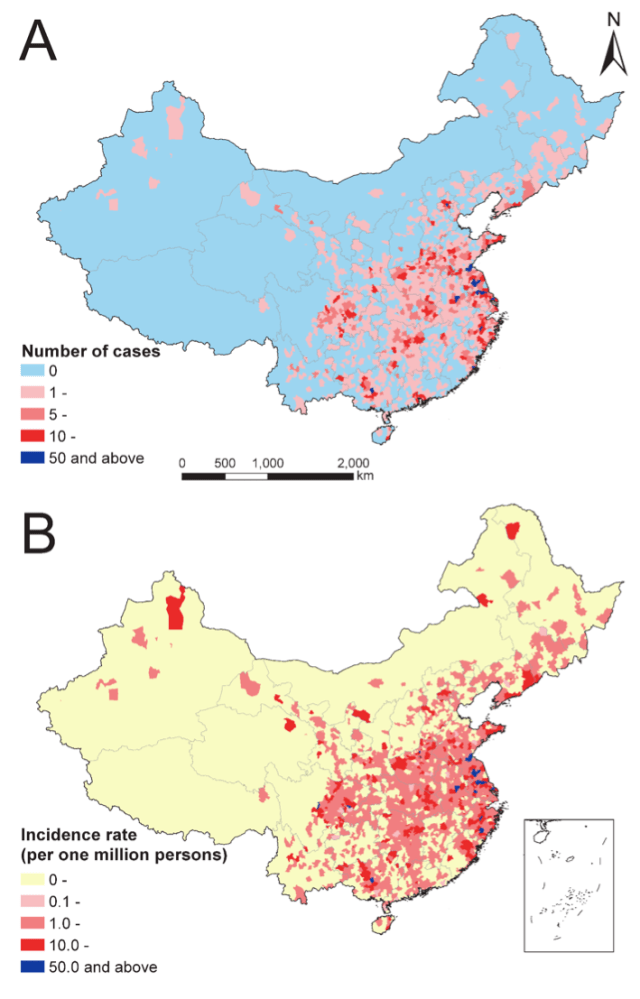
Figure 1. The distribution of imported P. Falciparium malaria cases by county in mainland China, 2011-2015. (A) Number of cases in mainland China (31 provinces). (B) Overall 5-year incidence rate per one million persons by county.
Connectivity and community of P. falciparum importation.
41 sub-Saharan countries exported P. falciparum into China, with Ghana (20.0%, 1734 cases), Angola (15.4%, 1333), and Nigeria (12.4%, 1076) being the top three origins. All 31 provinces in mainland China reported imported cases, with Guangxi (17.9%, 1548), Jiangsu (15.7%, 1355), and Henan (7.8%, 677) provinces as top three destinations. The median number of imported cases was 4 cases (IQR 2–11) for each origin-destination pair, and four distinct communities were identified in this imported malaria flow matrix. The first community included Ghana and Guangxi province: this link constituted the largest number of malaria case importations between SSA and Africa (1311 cases). The second community included five countries (Sudan, Ethiopia, Sierra Leone, Togo, and Rwanda) in Africa and two provinces (Xinjiang and Sichuan) in China; the third had ten countries with most in southern Africa and nine provinces with most in eastern China; others constituted the fourth community (Figure 2).
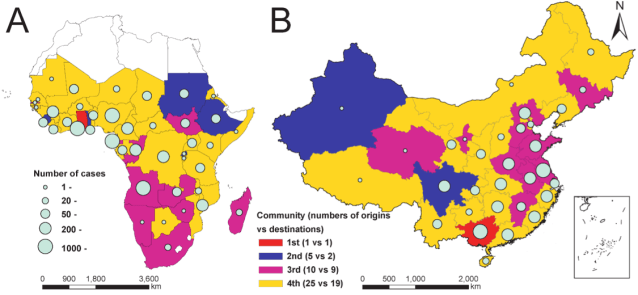
Figure 2. Four communities of origin-destination networks of P. Falciparium malaria importation from SSA to mainland China. (A) Origins (41 countries) in sub-Saharan Africa. (B) Destinations (31 provinces) in mainland China.
Driving factors of the importation phenomena.
According to Spearman‘s correlation coefficient, the number of P. falciparum cases exported from each SSA country to China was significantly associated with the volume of air passengers (median 2,080 persons, IQR 405-34,600; ρ=0.425, P=0.006), P. falciparum parasite prevalence estimates in 2-10 year-olds (PfPR2-10) in SSA (10.7%, 2.5%–30.6%; ρ=0.639, P<0.001), and total official development assistance (ODA) from China (610.4 million $, 219.7–4,654.0; ρ=0.679, P<0.001). By sector of ODA, significant correlations were found between the numbers of cases and investment in natural resource extraction (P<0.001), infrastructure (P=0.002), health (P=0.001), education (P=0.054), multi-sector (P=0.034), and “other” (P=0.011). Adjusting for the volume of air travelers and PfPR2-10, the quasi-Poisson regression model fitted by total ODA explained 65.9% (IQR 63.3%-69.8%) of the deviance of the number of cases in the training dataset, and 57.7% (23.7%-79.7%) in cross-validation. In the model, the total ODA and PfPR2-10 were positively correlated with numbers of cases with coefficients of 1.0 (IQR 0.96-1.13) and 0.70 (IQR 0.64-0.8), while volume of travelers had a negative coefficient of -0.45 (IQR -0.54 to -0.41).
Risk factors for deaths in imported cases.
The case-fatality rate was 11.3 per 1,000 cases (98 deaths in 8653 P. falciparum imported cases). The significant mortality risk factors identified by a multivariable logistic regression model were mainly related to the capacity of malaria diagnosis and socio-economic status of cases , including first-visit health institution at township level or lower (OR 2.6, 95%CI 1.5-4.2), more than 3 days between onset and diagnosis (2.2, 1.3-4.0), onset in January and February (2.3, 1.4-3.7), aged 50 years or older(2.4, 1.2-4.4), cases from provinces with GDP per capita of less than12,000 US$ (1.9, 1.0-3.9), low education (1.8, 1.0-3.3), and cases from communities 2nd to 4th identified by the network modularity analysis above.
The importation of malaria from Africa has been common over the past decades to non-endemic countries such as the USA, UK and France, that have historical, lingual and cultural ties with Africa., In particular, certain demographic groups exhibit substantially higher infection rates, such travelers visiting friends and relatives in endemic countries. However, as China has less historical, lingual or cultural ties with Africa- rather a relationship based on contemporary economic ties – male middle-aged migrant workers are the more dominant group exhibiting malarial infection. The data and analyses presented in this study highlight an emerging route of infectious disease importation for P. falciparum malaria from Africa to China. The volume of air travel from African countries to China, prevalence of malaria in origin countries and Chinese investments in African countries were all associated with the number and distribution of imported cases, with diverse risk factors for mortality found.
Strategies for targeting P. falciparum importation from SSA related to Chinese investment-related travel will likely be different from those that concentrate on local transmission in China. The evidence of this study, by mapping these emerging routes and defining drivers of parasite dispersal by human carriers, suggests that national malaria elimination programs should account for labour travel-mediated malaria spread. Interventions for reducing this importation pathway should communicate risks to travelers to alter their behaviors and improve regional capacity for diagnosis and treatment to prevent death. Strong surveillance systems need to be maintained to sustain the status of elimination in malaria-free regions by monitoring the risk of importation and the transmission potential in risk areas and form a cornerstone of post-2015 elimination strategies in China.
Shengjie Lai is a medical epidemiologist in the Division of Infectious Disease, Chinese Center for Disease Control and Prevention, and is a PhD student within the WorldPop team, the Department of Environment and Geography, the University of Southampton, UK. His research interests include population movements and infectious disease dynamics.
