
Cori Ruktanonchai presents maternal health outcomes at subnational level for five Sub Saharian African countries.
Maternal deaths across the globe have nearly been cut in half over the past 25 years, but for many of the world’s women, pregnancy and especially childbirth still remain fraught with peril. In much of East Africa alone, nearly 1 in 45 women risk death in order to give life, with the risk of dying as high as 1 in 20 for some countries. Furthermore, these risks are borne unequally, with those in rural and poor communities bearing a disproportionate burden. But how can we determine where mothers are least likely to obtain life-saving care throughout the spectrum of pregnancy? To address this question, we recently worked with policy makers from East African Community, the intergovernmental agency. In particular, we looked at geographic accessibility to maternal care in using advanced geographic information systems.
Using publicly available survey data, we modelled the odds throughout the region of: 1) skilled birth attendance, 2) receiving 4+ antenatal care visits at the time of delivery, and 3) receiving a postnatal health check-up within 48 hours of delivery. By combining these results with a comprehensive dataset of nearly 9,500 health facilities in the region, we mapped the probabilities of obtaining maternal and newborn health-care at both high-resolution and policy-relevant scales.
We found the odds of obtaining care were significantly reduced with increasing scores of geographic inaccessibility, with odds reduced by 25% and 75% for antenatal care, and skilled birth attendance, respectively. Overall, these results suggest that lower accessibility to the nearest health facility significantly deters utilisation of all maternal health care services. This study demonstrates how spatially-explicit approaches can inform policy efforts and promote evidence-based decision-making, and is particularly pertinent as the world shifts into the Sustainable Goals Development era, where sub-national applications will become increasingly useful in identifying and reducing persistent inequalities.
Maternal health and geography – an emerging perspective
The United Nations recently announced new Sustainable Development Goals (SDG) to reduce disparities in maternal health and promote health and well-being among women and children alike. Within this newly refurbished call for action is a particular emphasis on sub-national monitoring and geographically disaggregated health data. Fortunately, the last decades have seen advances in computational geostatistical techniques and an increasing availability of geo-located data. This means we now have the ability to produce fine spatial resolution maps, critical for uncovering previously overlooked geographical disparities.
Visualising geographic accessibility and maternal-newborn health care utilisation
To explore maternal and newborn health-care utilisation, we created a “gridded travel impendace surface”, essentially a digital map reflecting overall ease of traversing each 300 x 300 m square in the study region. We created this impedance surface for the study region by combining data on primary, secondary, and tertiary road networks, permanent water bodies and river networks via DIVA-GIS, land cover data from the European Space Agency’s 2009 GlobCover initiative , and elevation data from the Advanced Spaceborn Thermal Emission and Reflection Radiometer-Global Digital Elevation Model (ASTER-GDEM) Version 2. We subsequently used this impedance surface to perform a cost distance analysis, generating a geographic inaccessibility score for each 300 m grid cell, ranging from 0 (highly accessible) to 7 (highly inaccessible). The resulting scores represent ease of access to the nearest health facility, identified from a dataset of 9,314 facilities. These scores were then combined with information from the Demographic and Health Survey (DHS) for each cluster location. Finally, we visualized probabilities of obtaining maternal and newborn health-care (Uganda, Kenya, Tanzania, Rwanda and Burundi) (Figure 1)
Using maps to inform policy efforts
We found that increasing geographic inaccessibility to the nearest health facility was associated with the greatest reduction in odds of utilising maternal and newborn health-care, particularly among skilled birth attendance (SBA: 0.24; 95% CI: 0.19 to 0.30; ANC: 0.74; 95% CI: 0.61 to 0.89; PNC: (0.58; 95% CI: 0.45 to 0.75). To visualise where women were least likely to obtain these critical services, we mapped probabilities of maternal and newborn health-care at a 300 x 300 m resolution.
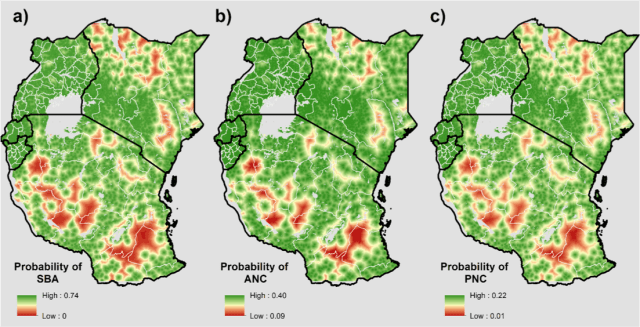
Figure 1: Probability (300 m x 300 m) of a) delivery with Skilled Birth Attendance (SBA) present, b) four or more antenatal care (ANC), and c) postnatal care (PNC) received within 48 hours of delivery in Uganda, Kenya, Tanzania, Rwanda, and Burundi.
A nuanced understanding of how geographic accessibility influences uptake of maternal and newborn health-care at a very fine spatial resolution will be key to identify and reduce these inequalities and alleviate coverage gaps. Often, however, policy decisions are made at a subnational scale with meaningful administrative units, such as districts or states. Therefore to promote policy relevance, we aggregated these high-resolution surfaces to the administrative unit II scale (this typically refers to districts, but varies by country) and adjusted probabilities by number of live births per administrative unit to more accurately reflect actual births at-risk.
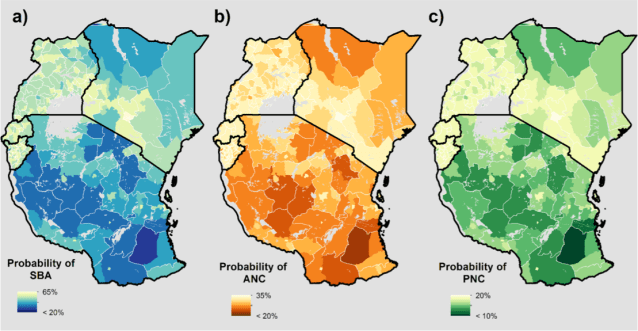
Figure 2: Probability (admin II) of a) delivery with a skilled birth assistance (SBA), b) four or more antenatal care (ANC) visits at time of delivery, and c) postnatal care (PNC) received within 48 hours of delivery.
Regionally, we found that Kenya and Tanzania had the strongest patterns of spatial heterogeneity in the observed outcomes and generally lower probabilities of obtaining all types of care. The lowest probabilities observed were throughout rural districts in northern Kenya and central Tanzania. Conversely, we found Rwanda and Burundi to have generally higher probabilities of obtaining care, as compared to Tanzania, Kenya, and Uganda. This trend could be due in part to the relative density of facilities available, while more remote areas of Kenya and Tanzania have comparatively less facilities and primary or secondary road networks. This pattern also occurred sub-nationally, as we observed higher probabilities of obtaining care in urban versus rural districts, indicating infrastructure density is important in increasing maternal and newborn health-care coverage. Similar findings for Kenya have been reported before in this blog post.
These findings suggest the allocation of funds on infrastructure, such as buildings, equipment, and health workers, should appropriately reflect the demography and epidemiology of the area. These analyses could help to direct the flow of such resources, by highlighting areas and populations where care utilisation rates are lowest.
A new era of maternal health
With the growing computational power and availability of spatially explicit data, these analyses represent a new and emerging frontier for maternal health. Importantly, moving forward within the new Sustainable Development Goal era will necessitate open access data and findings to inform policy efforts and drive innovative new research and insights. Towards this end, the data we used to inform our research and our subsequent findings are made freely available through the WorldPop project. Also available through WorldPop are the births and pregnancies’ estimates used in these analyses at a 100 x 100 m resolution, along with other high resolution surfaces including population dynamics and spatial demographics such as literacy and poverty. For further spatial visualizations of key maternal health outcomes and indicators, be sure to also check out www.atlasofbirth.org, soon to be available through the University of Southampton.
Cori Ruktanonchai is a PhD student within the WorldPop team, and is based in Geography & Environment and Social Statistics at the University of Southampton. This blog post is based on her article published in the Maternal Health Taskforce’s PLoS ONE special collection, Neglected Populations: Decreasing Inequalities & Improving Measurement in Maternal Health. Cori received a Masters in Public Health at the University of Florida, and currently focuses on utilising spatially explicit approaches to investigate high-resolution maternal and newborn health outcomes in East Africa. This work was funded through the Norwegian Development Agency (NORAD), grant number RAF-2946 RAF-12/0094, in collaboration with ICS Integrare. Cori is supported by the University of Southampton’s Economic and Social Research Council’s Doctoral Training Centre.
